1. Elbow epicondylitis
2. Ulnar neuritis
3. Olecranon bursitis
4. Locking/Clicking Elbow
5. Distal biceps tendon rupture
6. Posterior Impingement of Elbow
7. Elbow fractures
8. Elbow Dislocations – Instability
9. Arthritis of the Elbow
1. Elbow epicondylitis
Tennis Elbow
Tennis elbow is a chronic inflammation of a tendon of the outside of the elbow. It is also known as ‘lateral epicondylitis’ .

Cause:
The exact cause of tennis elbow is not known, but it does tend to occur after repetitive use of the extensor tendons at the elbow, originating from the Extensor Carpi Radialis (ECRB) tendon , such as in tennis (hence the name). These tendons are involved in extending the wrist joint and is also active when gripping with the wrist extended (as in tennis). Any activity that twists and extends the wrist can lead to tennis elbow.
The tendons become chronically irritated and worn. This leads to the pain with activities.
Presentation:
The first sign of tennis elbow is usually tenderness and pain when pressure is applied to the outside of the elbow. If left untreated, a dull constant pain or sharp shooting pain can be felt. Swelling may be present. Other symptoms include:
Pain when the wrist or hand is straightened (wrist extension)
Pain felt when lifting a heavy object
Pain when making a fist or shaking hands
Shooting pains from the elbow down to the forearm or up into the upper arm
Pain with tennis elbow is typically localised over the bony bump on the outside of the elbow (lateral epicondyle) and may extend down to the hand. This area is usually very tender to touch. Rest usually relieves the pain.
Sometimes other conditions that are not linked to tennis elbow can cause pain in the elbow. For example, arthritis of the elbow, a pinched nerve in the neck, shoulder impingement and carpal tunnel syndrome.
Treatment:
The type and duration of the treatment will depend on the severity of the condition. The first step in treating tennis elbow is to manage the activities that cause the pain, such as tennis or golf.
Pain killers and anti-inflammatory medications relieve the pain and reduce the inflammation.
A tennis elbow strap can be worn just below the elbow to limit the stress on the ECRB tendon.
Treating the area with an ice pack and performing an ice massage are also recommended.
Physiotherapy to release the tendon inflammation and retrain the extensor muscles is important. Eccentric exercise programs are popular and prove effective in 70% of cases.
Injections: If the condition does not respond to the above treatments, injections are often used. Steroid injections are the most commonly used injections, but they generally wear off after a few months and may need repeating. More recently Platelet Rich Plasma (PRP) injections have shown to be more effective than steroid injections.
Surgery: For very severe cases and those that fail to improve after injections surgery may be necessary. The surgery is usually performed as day case surgery. This may be performed by an open minimally invasive approach. There are pros and cons to each of these methods, but the results are similar. You will be able to start moving your elbow normally two days after the surgery, with 1 week off work. Full recovery may take three months.
Prevention:
To prevent tennis elbow from reoccurring, it is important to make sure you keep the muscles strong by exercise and using the proper form whether playing tennis or lifting heavy objects. Warming up before starting to use the muscle will also help prevent the condition. After exercising, you may want to ice and stretch the elbow and arm muscles.
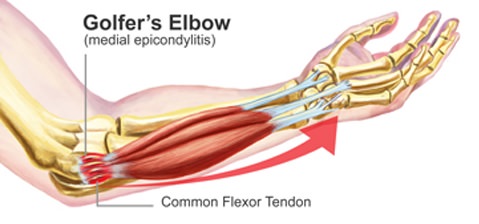
Golfer’s Elbow
Golfer’s elbow is a chronic inflammation of a tendon of the inner side of the elbow. It is also known as ‘medial epicondylitis’.
Cause:
The exact cause of golfers elbow is not known, but it does tend to occur after repetitive use forearm and wrist. It is does not only affect golfers. The causes are similar to Tennis Elbow
Presentation:
Pain over the bony prominence on the inner side of the elbow. The pain can extend down the forearm to the wrist and hand. The pain is made worse by bending the wrist and grasping objects tightly. There may be discomfort in extending (straightening) the wrist also, due to stretching of the affected flexor muscles.
Treatment:
The type and duration of the treatment will depend on the severity of the condition. The treatments are similar to Tennis Elbow.
The first step in treating golfers elbow is to eliminate the activities that cause the pain, such as tennis or golf.
Pain killers and anti-inflammatory medications relieve the pain and reduce the inflammation.
A forearm strap can be worn just below the elbow to limit the stress on the muscles.
Treating the area with an ice pack and performing an ice massage are also recommended.
Physiotherapy to release the tendon inflammation and retrain the muscles with eccentric exercises.
Injections have may be used. Steroid injections are the most commonly used injections, but they generally wear off after a few months and may need repeating. More recently Platelet Rich Plasma (PRP) injections have shown to be more effective than steroid injections, but are much more expensive.
If the condition does not respond to the above treatments, surgery may be necessary. The surgery is usually performed as day case surgery. This may be performed by an open minimally invasive approach.
You will be able to start moving your elbow normally two days after the surgery, with 1 week off work. Full recovery may take three months.
Prevention:
To prevent golfers elbow from reoccurring, it is important to make sure you keep the muscles strong by exercise and using the proper form whether playing sports or lifting heavy objects. Warming up before starting to use the muscle will also help prevent the condition. After exercising, you may want to ice and stretch the elbow and arm muscles.
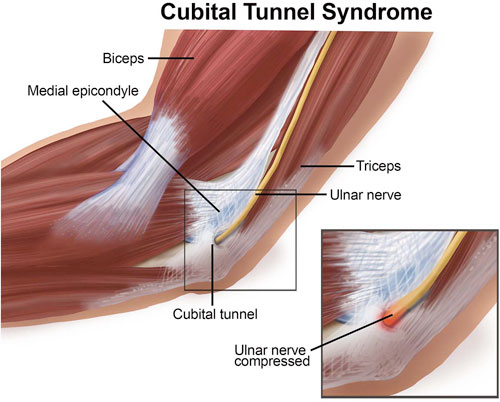
2. Ulnar neuritis
Ulnar neuritis is an inflammation of the ulnar nerve as it passes on the inside of the elbow down to the forearm and hand. It can also be known as ulnar nerve compression or cubital tunnel syndrome. It is common in throwing athletes, although it can be seen in active people and even non-active people.
People with irritation or compression of the ulnar nerve will often notice numbness and tingling in their ring and little fingers with activity or even at rest. Occasionally the athlete will notice soreness or a dull pain on the inside of the elbow and forearm. In long-standing symptoms, weakness with grip in the hand can be noted.
The ulnar nerve runs behind the medial epicondyle on the inside of the elbow. The surgeon often can make this diagnosis by physical exam in the office. Tapping the ulnar nerve as it lies just behind the bony process on the inside of the elbow (people often think of it as hitting the “funny bone”) will reproduce the symptoms. Tapping the nerve can cause a pins and needles sensation on the inside of the elbow or down into the fourth and fifth fingers. Also weakness with grip can be noted as well. The physician will also check for other causes of medial elbow pain as well as instability to valgus stress, which could signify ulnar collateral ligament deficiency in a throwing athlete. X-rays are usually unremarkable, but physicians often order nerve conduction studies. These are studies that test the action of nerve signals. These tests can identify compression of the ulnar nerve and where the nerve is compressed to help plan treatment.
Initially, rest or avoiding offending activities, anti-inflammatory medications, and the patient’s wearing a night splint can be attempted. Long-standing or significantly disabling cases often require surgery. Surgery can simply involve decompression of the nerve on the inside of the elbow. Occasionally moving the nerve in front of the medial epicondyle is needed, especially if the patient has a snapping sensation where the nerve slides back and forth across the medial epicondyle area.
Return to sports depends on resolution of symptoms and the type of treatment needed. If it resolves without surgery or with a simple decompression, return to sports can be fairly quick. Transposition of the ulnar nerve often requires a longer period of time to get back to sports.
3. Olecranon bursitis
Bursae are thin, slippery sacs located throughout the body that act as cushions between bones and soft tissues. They contain a small amount of lubricating fluid that allows the skin to move freely over the underlying bone. The olecranon bursa lies between the loose skin and the pointy bone at the back of the elbow called the olecranon.

Normally, the olecranon bursa is flat. If it becomes irritated or inflamed, more fluid will accumulate in the bursa and bursitis will develop.In elbow bursitis, the bursa fills with fluid, causing pain and limiting movement.
Elbow bursitis can occur for a number of reasons.
Trauma: A hard blow to the tip of the elbow can cause the bursa to produce excess fluid and swell.
Prolonged pressure: Leaning on the tip of the elbow for long periods of time on hard surfaces, such as a tabletop, may cause the bursa to swell. Typically, this type of bursitis develops over several months.
People in certain occupations are especially vulnerable, particularly plumbers or heating and air conditioning technicians who have to crawl on their knees in tight spaces and lean on their elbows.
Infection: If an injury at the tip of the elbow breaks the skin, such as an insect bite, scrape, or puncture wound, bacteria may get inside the bursa sac and cause an infection. The infected bursa produces fluid, redness, swelling, and pain. If the infection goes untreated, the fluid may turn to pus. Occasionally, the bursa sac may become infected without an obvious injury to the skin.
Medical conditions: Certain conditions, such as rheumatoid arthritis and gout, are associated with elbow bursitis.
Swelling is often the first symptom. The skin on the back of the elbow is loose, which means that a small amount of swelling may not be noticed right away. In many cases, the first sign of bursitis is swelling at the elbow. As the swelling continues, the bursa begins to stretch, which causes pain. The pain often worsens with direct pressure on the elbow or with bending the elbow. The swelling may grow large enough to restrict elbow motion. If the bursitis is infected, the skin becomes red and warm. If the infection is not treated right away, it may spread to other parts of the arm or move into the bloodstream. This can cause serious illness. Occasionally, an infected bursa will open spontaneously and drain pus.
The diagnosis is always clinical and an x-ray is recommended in order to look for a foreign body or a bone spur. We may need to take a small sample of bursa fluid with a needle to diagnose whether the bursitis is caused by infection or gout. Blood tests are not usually helpful.
Treatment
Nonsurgical Treatment
We may recommend aspirating (removing the fluid from) the bursa with a needle. This is commonly performed as an office procedure. Fluid removal helps relieve symptoms and give us a sample that can be looked at in a laboratory to identify if any bacteria are growing. This also let us know if a specific antibiotic is needed to fight the infection. We may prescribe antibiotics before the exact type of infection is identified. This is done to prevent the infection from progressing.
If the bursitis is not from an infection, it is treated with a number of options.
Elbow pads. An elbow pad may be used to cushion your elbow.
Activity changes. Avoid activities that cause direct pressure to your swollen elbow.
Oral medications such as ibuprofen or other anti-inflammatories may be used to reduce swelling and relieve your symptoms.
If swelling and pain do not respond to these measures after 3 to 4 weeks, we may recommend removing fluid from the bursa and injecting a corticosteroid medication into the bursa. The steroid medication is an anti-inflammatory drug that is stronger than the medication that can be taken by mouth. Corticosteroid injections usually work well to relieve pain and swelling. However, symptoms can return.
Surgical Treatment
Surgery for infected bursa. If the bursa is infected and it does not improve with antibiotics or by removing fluid from the elbow, surgery to remove the entire bursa may be needed. This surgery may be combined with further use of oral or intravenous antibiotics.
The bursa usually grows back as a non-inflamed, normally functioning bursa over a period of several months.
Surgery for noninfected bursa. If elbow bursitis is not a result of infection, surgery may still be needed if nonsurgical treatments do not work. In this case, surgery to remove the bursa is usually performed as an outpatient procedure. The surgery does not disturb any muscle, ligament, or joint structures.
After surgery we will apply a splint to your arm to protect your skin. In most cases, casts or prolonged immobilization are not necessary. Although formal physical therapy after surgery is not usually needed, we will recommend specific exercises to improve your range of motion. These are typically permitted within a few days of the surgery. Your skin should be well healed within 10 to 14 days after the surgery, and then you will be able to fully use your elbow. Your elbow may need to be padded or protected for several months to prevent reinjury.
4. Locking/Clicking Elbow
Locking and/or painful clicking of the elbow joint is usually due to ‘loose bodies’ or arthritis of the elbow. The loose bodies are usually bits of the cartilage lining of the joint which break off and float in the joint. In certain positions they can cause the joint to click or lock. Sometimes they may only cause pain, similar to tennis elbow. An x-ray or scan may be required to tell the difference. Loose bodies can usually be removed by arthroscopic surgery.

5. Distal biceps tendon rupture
The biceps muscle is the large muscle in the front of your upper arm. It is the muscle most flexed by strongmen in demonstrating their muscles. The biceps is attached at the top in the shoulder and then below the elbow into the radius bone by a strong tendon.
This strong tendon at the elbow can rupture with a very strong contraction of the biceps muscle. People may feel a pop in the elbow and pain. This usually happens when the tendon is already worn and prone to injury.

Distal biceps tendon rupture:
The people most likely to get a biceps tendon rupture are strength athletes, bodybuilders and heavy manual workers. Generally, males over the age of 35 years. Unlike other tendon ruptures, steroid use has not been shown to be involved in the rupture of the distal biceps.
After the injury there is usually localised pain at the front of the elbow, with bruising and swelling. The biceps muscle may retract up the upper arm crating a prominent bump, known as the ‘Popeye’ sign. This is often visibly different to the other biceps when contracting the muscle.
A biceps tendon rupture leads to weakness of the elbow and forearm if not repaired. People have difficulty twisting a screwdriver, turning a key and lifting weights. This is due to 55% reduction in forearm twisting strength (supination power) and 36% reduction in elbow bending strength (flexion power).
Therefore, early operative repair is the treatment of choice to restore full strength and correct the deformity. Repair should be undertaken within 3 weeks of the injury, or as early as possible.
There are many different repair techniques. I prefer a small approach and repair with strong bone anchors, reattaching the tendon down to the bone. The repair is strong and patients can start moving soon after the surgery. However lifting must be avoided for at least 6 weeks after surgery.

A biceps tendon rupture that is over 4 weeks old is often more difficult to repair directly. The tendon is often retracted up the arm and stuck, so a second higher incision may be made to retrieve it. Sometimes a reconstruction with another tendon might be required. In such chronic cases we ‘bridge’ the repair and reinforce it with either tendon from the patient’s thigh (tensor fascia lata) or a tendo-achilles allograft.
6. Posterior Impingement of Elbow
Posterior impingement is due to over use and repetitive forced extensions of the elbow. This may occur during sports, such as overhead racket sports, throwing, swimming and boxing. With repeated extension (straightening of the elbow), the olecranon tip is repeatedly jammed into the fossa at the back of the elbow, which results in inflammation of the joint lining (synovium), proceeding to injury to the cartilage and bone. Bone spurs may sometimes form on the tip of the olecranon leading to further injury and soft tissue impingement. There becomes increased risks of impaction and injury when there are shearing forces that occur as at result of a valgus strain (strain that opens up the inner side of the elbow), such as during serving and hitting topspin forehands with an extreme wrist and grip in tennis; similarly, this may occur with badminton.
The typical symptoms are pain and tenderness at the back of the elbow, especially when trying to throw, straighten the elbow, or during serving and overhead racket shots. This may proceed to locking and a catching of the elbow. There may be swelling of the elbow and inability to serve at full speed. There may be some elbow stiffness and towards the late stages an inability to fully straighten the elbow.
Investigations such as x-rays may not adequately reveal the diagnosis unless there are spurs or loose bodies in the back of the elbow. Ultrasound scan and MRI scan may be useful in expert hands.

Posterior impingement syndrome of the elbow is often treatable with non-operative management. A rehabilitation programme to improve strength, flexibility and elbow range of motion may be helpful. Injections into the posterior compartment (back) of the elbow are often useful to reduce the inflammation and swelling, either Cortico- steroids or Hyaluronons may be used. When non-operative measures have failed or particularly if there is locking and catching due to loose bone fragments within the joint and spurs, arthroscopic (keyhole) surgery is required to remove them. Return to sports after this surgery may take up to 3 months.
7. Elbow fractures
Elbow fractures may result from a fall, a direct impact to the elbow, or a twisting injury to the arm. Sprains, strains or dislocations may occur at the same time as a fracture. X-rays are used to confirm if a fracture is present and if the bones are out of place. Sometimes a CT (Computed Tomography) scan might be needed to get further detail.
The different types of elbow fractures include:
Radial head and neck fractures
Pain is usually worse with forearm rotation (turning the palm up and down). The treatment for this fracture depends on the number and size of the bone fragments. Complex fractures often require surgery to repair and stabilize the fragments or to remove or replace the radial head if there are too many bony pieces.

Olecranon fractures
These fractures are usually displaced and require surgery. The bone fragments are re-aligned and held together with pins and wires or plates and screws.

Fractures of the distal humerus
These fractures occur commonly in children and in the elderly. Nerve and/or artery injuries can be associated with these types of fractures and must be carefully evaluated by your doctor. These fractures usually require surgical repair with plates and/or screw, unless they are stable.
Symptoms:
Pain, swelling, bruising and stiffness in and around the elbow may be signs of a possible fracture. A snap or pop at the time of injury may be felt or heard. Visible deformity might mean that the bones are out of place or that the elbow joint is dislocated. There may be numbness or weakness in the arm, wrist and hand.
Treatment:
Non-surgical treatment such as using a sling, cast or splint is typically used when the bones are at low risk of moving out of place or when the position of the bones is okay as is. Age is also an important factor when treating elbow fractures. Casts are used more frequently in children, as their risk of developing elbow stiffness is small; however, in an adult, elbow stiffness is much more likely.
Surgical treatment: Fractures that are out of place or unstable are more likely to require surgery. A surgical procedure would replace and stabilize the fragments or remove bone fragments. Whenever a fracture is open (skin broken over the fracture), urgent surgery is needed to clean out the wound and bone to minimize the risk of infection.
Rehabilitation is used to maximize motion and decrease the chance of getting elbow stiffness. This might include exercises, scar massage, ultrasound, heat, ice and splints that stretch the joint.
8. Elbow Dislocations – Instability
Dislocations of the elbow need to be reduced urgently. If there is still instability and/or fractures these need to be treated early to prevent long-term problems. The range of injuries in the elbow associated with a dislocation is complex and requires expert management.
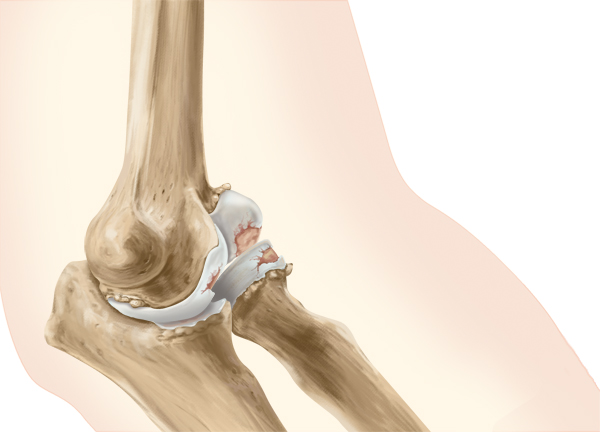
9. Arthritis of the Elbow
Arthritis of the elbow can cause pain not only when they bend their elbow, but also when they straighten it, such as to carry a briefcase. The most common cause of arthritis of the elbow is rheumatoid arthritis. Osteoarthritis and injuries can also cause arthritis in the elbow joint.
Rheumatoid arthritis is a disease of the joint linings, or synovia. As the joint lining swells, the joint space narrows. The disease gradually destroys the bones and soft tissues. Usually, RA affects both elbows, as well other joints such as the hand, wrist and shoulder.
Osteoarthritis affects the cushioning cartilage on the ends of the bones that enables them to move smoothly in the joint. As the cartilage is destroyed, the bones begin to rub against each other. Loose fragments within the joint may accelerate degeneration.
Trauma or injury to the elbow can also damage the cartilage of the joint. This can lead to the development of arthritis in the injured joint.
Symptoms of elbow arthritis vary.
In the early stages of rheumatoid arthritis, pain may be primarily on the outer side of the joint. Pain generally gets worse as you turn (rotate) your forearm. The pain of osteoarthritis may get worse as you extend your arm. Pain that continues during the night or when you are at rest indicates a more advanced stage of osteoarthritis.
Swelling is more common with rheumatoid arthritis.
The joint isn’t stable and gives way, making it difficult or impossible to do normal daily activities.
Lack of full movement. You are not able to straighten (extend) or bend (flex) the elbow.
Locking. Your elbow joint catches or locks. This can happen with osteoarthritis.
Stiffness. This happens particularly with arthritis that develops after an injury.
Diagnosis
During a physical examination, we will first look for tenderness and swelling. We will also look at the range of motion you have as well as identifying what positions cause pain to your elbow joint. X-rays often show the joint narrowing as well as any loose bodies (e.g., bony pieces). If your pain is due to arthritis following an injury, the X-ray may show an improper joining or a failure to join of the elbow bones.
Treatments
Nonsurgical Treatment
The first treatments used for elbow arthritis include:
Cut back on activity. Osteoarthritis may be caused by the repetitive overuse of the joint. Avoiding certain activities or sports may be helpful. Having periods of rest after exercise or activity involving your elbow can relieve stress on the joint
Pain management. Acetaminophen or ibuprofen can provide short-term pain relief. More powerful drugs may be prescribed to treat rheumatoid arthritis. These include anti-malarial agents, gold salts, drugs that suppress your immune system and corticosteroids. An injection of a corticosteroid into the joint can often help.
Physical Therapy. Applying heat or cold to the elbow and gentle exercises may be prescribed. A splint to protect the elbow from the stress of moving may be helpful. Devices that reduce stress on your joints such as handle extensions, to maintain daily activities.
Surgical Treatment
If arthritis does not respond to other treatments, surgery may be discussed. The specific type of surgery may depend on the type of arthritis, the stage of the disease, your age, your expectations and your activity requirements.
Surgical options include:
- Arthroscopy. Using special instruments and two or three small incisions, we can remove bone spurs, loose fragments or a portion of the diseased synovium. This procedure can be used with both rheumatoid arthritis and osteoarthritis.
- OK procedure. The OK procedure is used to remove loose bone from inside the elbow or to improve pain and movement for a stiff elbow. This procedure has been described to treat mild to moderate osteoarthritis of the elbow.

- A total joint replacement is usually reserved for patients over 60 years old or patients with RA, osteoarthritis or traumatic arthritis in advanced stages.

