1. Shoulder Dislocation – Instability
2. Impingement syndromes
3. Rotator Cuff Tears
4. Calcific tendonitis
5. Frozen Shoulder
6. Biceps Problems
7. Acromioclavicular Joint
8. SLAP Lesions
9. Fractures
10. Arthritis of the Shoulder
1. Shoulder Dislocation – Instability
The shoulder joint is stabilised by the shoulder labrum and capsule (as well as the surrounding muscles).
The labrum is a cartilage-like ring surrounding the glenoid.
The capsule is a series of ligaments that connects the humerus to the glenoid.
When the labrum and/or ligaments stetch or tear, the shoulder has a greater tendency to dislocate. This is known as instability, which can lead to greater and more painful shoulder conditions, especially dislocation and subluxation.
Dislocation and subluxation are the telltale signs of instability .
The shoulder may dislocate either out the front (anterior), out the back (posterior) or out the bottom (inferior – subluxio erecta).

Shoulder instability means your shoulder can dislocate or subluxate repeatedly during active movement or exercise. Subluxate means the joint moves more than it should do in normal circumstances but doesn’t actually come out of joint. There can be a number of reasons for this and this will determine the type of treatment you will receive.
Shoulder instability is divided into three main categories (this is largely dependant on the first episode of dislocation).
- Traumatic dislocation
This when the shoulder has undergone an injury with enough force to pull the shoulder out of joint such as being tackled in a football or rugby game, a road traffic accident etc. Usually this is the first episode and it would need reducing in A&E. You would be put into a sling for a period of time and then in some cases would undergo a course of physiotherapy. Due to the amount of force that is associated with such an injury the labrum can be torn from the bone (creating a Bankart lesion .) and this can result in an unstable shoulder which may lead to further episodes of dislocation. This would be an indication for a surgical procedure called an Anterior Stabilisation where the torn part of the labrum ( Bankart lesion ).

A Bankart lesion is the most common injury sustained with traumatic dislocation, but other injuries can occur. These may alter the surgery and rehabilitation. These injuries can usually be diagnosed on an MR-Arthrogram or CT-Arthrogram.
These injuries are:
- ALPSA lesion – (Anterior Labral Periosteal Sleeve Avulsion) a displacedBankart tear, where the labrum has displaced around the glenoid neck. This is associated with a higher risk of recurrent instability than an undisplacedBankart tear.
- HAGL tear – (Humeral Avulsion of Glenohumeral ligament)
- Bony Bankartt – a fragment of bone breaks off with the Bankart tear
- Hill-Sachs lesion – a dent in the back of the humeral head which occurs during the dislocation as the humeral head impacts against the front of the glenoid.
- SLAP Tear – a tear at the top of the labrum
- Atraumatic dislocation
This occurs when the shoulder dislocates with minimal force such as reaching up for an object or turning over in bed. Usually it will ‘pop’ back in itself or with a little help. Normally this type of dislocation does not need reducing in A&E. It can occur regularly throughout the day and will be associated with certain positions the arm is placed into. This type of dislocation is associated with people that have ‘lax’ joints, for example people who hyper-extend their knees and elbows and can get the palms of both hands onto the floor with ease. This joint laxity is normal for these people and the onset of dislocation can be associated with a change in how the muscles around the shoulder are interacting with each other or a change in posture/ position of the arm. This can produce an imbalance in the control of the joint. Referral for appropriate physiotherapy is the initial form of management. The physiotherapist should look at the way in which the muscles and shoulder joint is moving and posture aiming to restore the balance. Treatment can ‘cure’ the problem as long as the exercises and advice is continued, but in some cases there is only minimal or nil benefit. At this point surgical intervention is indicated.
- Positional Non-traumatic dislocations
This group of people can dislocate their shoulders without any form or history of trauma. Some may have started out dislocating their shoulder as a party trick; others may have always had shoulders that just ‘fall’ out of joint. This type of dislocation is usually painless and can be put back in easily. Both shoulders are typically involved. The cause of this type of dislocation is usually a result of what we call ‘abnormal muscle patterning’ which means the strong muscles around the shoulder joint are not working in the correct order causing them to pull the shoulder out of joint with active movement in the particular direction such as lifting the arm forward above the head or out to the side and above the head. The main treatment for this is physiotherapy that looks at re-sequencing the muscles in order to prevent further dislocations. Occasionaly surgery in the form of thermal capsular shrinkage or plication may be neccessary.
Treatment
Physiotherapy – to train the shoulder muscles to control the shoulder correctly and prevent further instability
Surgery – A number of procedures are available to remedy chronic instability, depending on the causes and findings on investigations.
Types of Surgery:
Arthroscopic Procedures – through keyhole surgery.
Open Shoulder Procedures – depending on the problems found, such as the Latarjet procedure for glenoid bone loss or open capsular repair for HAGL lesions.
Prevention
Strong shoulder muscles remain the best defence against shoulder dislocation, subluxation, and, thus, instability. Exercises that build up these muscles around the shoulder should be done. The key is to balance the muscles around the shoulder and ensure not only the ‘mirror’ muscles are exercises (those that you can see when looking in the mirror). Good core stability and posture are also important.
Adequate warm-up before activity and avoidance of high-contact sports will help prevent instability-causing injuries.
2. Impingement syndromes
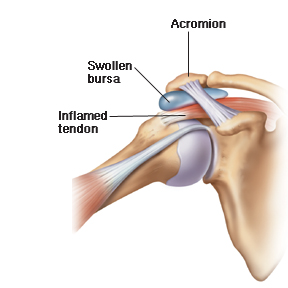
Subacromial Impingement
The four muscles that raise and lower the arm (and their respective tendons) are collectively known as the rotator cuff . The rotator cuff lies under the roof of the shoulder (an extension of the shoulder blade known as the acromion ). The space between the acromion and the rotator cuff tendons is filled by the subacromial bursa . This bursa is a fluid filled sac that allows for smooth gliding of the rotator cuff under the acromion with overhead movements of the shoulder.
The rotator cuff works a depressor and centraliser of the humeral head in the glenohumeral joint. As the arm is elevated the rotator cuff depresses the humeral head allowing it to glide easily underneath the acromion.
Should any abnormality occur affecting the rotator cuff this would lead to dysfunction of the rotator cuff. Therefore as the arm is elevated, the depressing and centralising effect would be lost and the humeral head would ride upwards closer to the acromion at risk of causing impingement.
Pathologies that could do this are those directly affecting the rotator cuff such as:
- Rotator cuff strain
- Partial or full thickness tear
- Calcific tendonitis
- A tendonopathy due to chronic overuse.
Indirect causes:
- Glenohumeral instability
- Labral tears, in particular SLAP tears
- Abnormal muscle patterning problems of the shoulder.
The acromion differs in individuals normally (morphological variants). These were described by Bigliani as type I, type II or type III. Type I is flat, type II is curved and type III hooked. A person with a type II or type III acromion would be at a higher risk of impingement due to the narrowing of the acromiohumeral gap and bursal space.
In addition to the above, with advancing age people tend to develop a bone spur on the front and side of the acromion. This further reduces the subacromial space increasing the risk of impingement.
The rotator cuff and acromion will then rub against one another, causing a painful condition known as impingement. Each time the arm is raised there is a bit of rubbing on the tendons and the bursa between the tendons and the acromion, which may cause pain and inflammation.
Impingement may become a serious problem for some people and disturb their normal activities. This is when treatment is needed.
Treatment of impingement syndrome involves:
1. Painkillers and anti-inflammatory medications
2. Physiotherapy – the key part of management to work on good posture, shoulder blade positioning and strengthening of the weakened rotator cuff muscles
3. Injections – reduces inflammation and control the pain, allows the rotator cuff muscles a chance to recover and improve with the exercises
4. Surgery – the goal of any surgery to reduce the effects of impingement, by increasing the amount of space between the acromion and the rotator cuff tendons, which will then allow for easier movement and less pain and inflammation. The operation performed is Arthroscopic Subacromial Decompression (ASD)
Prevention
Avoid excessive overhead activities.
Strengthen your shoulders and do not try to play or work through the pain.
Internal Impingement
The condition is mainly seen in athletes, where overhead activity is a major part of their sport, particularly throwing athletes. In-fact, the condition is sometimes called “The Throwers Shoulder” and is also seen in the “Swimmer’s Shoulder”. It is for this reason that it is mainly seen in a younger athletic population.
Internal impingement involves structures within the main shoulder joint itself (Glenohumeral joint).
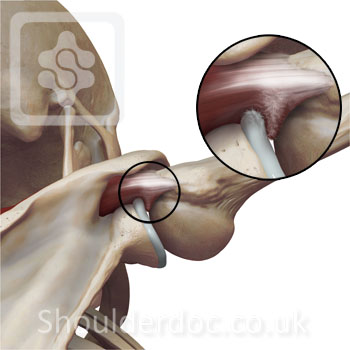
The combination of abduction and external rotation in the cocking phase of throwing causes an impingement of the underside of the rotator cuff against the posterior (back) superior (top) labrum.
Image showing how the rotator cuff gets ‘pinched’ (impinged) between the glenoid labrum and the humeral head in full abduction and external rotation.
This is something which occurs to everyone during throwing. Therefore internal impingement in itself is not an injury. It becomes an injury when over time, microtrauma from repetitive throwing results in damage to the rotator cuff (see rotator cuff tears) or the superior portion of the labrum (see SLAP tears).
The ‘impingement’ lesions on the labrum and rotator cuff are known as ‘kissing lesions’. The image below shows a view of the lesions at arthroscopy (viewing from anterior):
Symptoms
The main symptom patients with internal impingement usually complain of is pain. This is usually made worse by over-head activity or throwing. The pain is a result of inflammation and irritation to the tendons which are being impinged. This is called a tendonitis. Also affected is the bursa. This is a fat pad within the shoulder to allow tendons and muscles to glide over bones easily. If this becomes inflamed and irritated it is called bursitis. There may also be shoulder instability as a result of the damage done to the labrum. The damage done to the rotator cuff may cause a weakness in the movements of the shoulder, particularly abduction and external rotation, the movements discussed above as being crucial to throwing.
Diagnosis
Internal impingement is usually diagnosed on clinical examination.
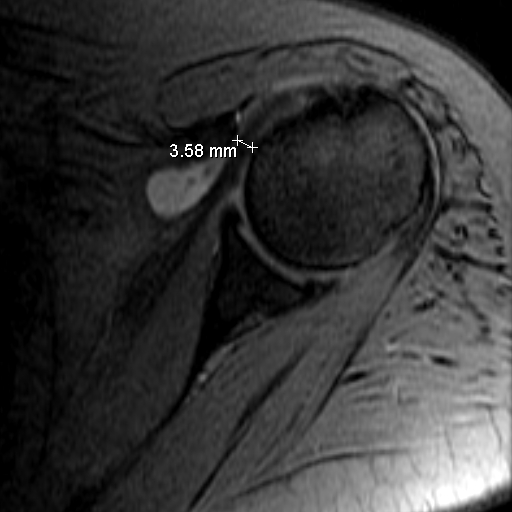
Special tests such as a MR arthrogram may be useful. This is a specific type of MRI scan in which a dye is injected into the joint space to allow tears in the labrum to be seen. Fluid around tendons and in the joint could also point to impingement. It may also show up tears in the rotator cuff. Similar things may also be picked up on an ultrasound scan
Treatment
Treatment can be divided into five phases:
Rest: This allows inflammation in the tendons, joint capsule and bursa to subside.
NSAIDS and steroid injection: To help facilitate the decrease in inflammation, NSAIDs such as ibuprofen can be helpful, as can a steroid injection into the joint
Strengthening programme: Aimed at the rotator cuff muscles and other muscles of the shoulder and upper back.
Sports / Job specific training: Rehab aimed at a specific area of performance; in this case it is likely to be throwing.
Surgery: If rehab fails to provide satisfactory results then surgery is indicated. This is aimed at repairing rotator cuff damage or labral damage. If the rotator cuff is badly damaged, then early repair must be considered. Controlled ‘rebalancing’ of the capsule may also be performed.
Subcoracoid Impingement
Subcoracoid impingement is an unusual form of shoulder impingement results from narrowing of the coracohumeral interval (space between the tip of the coracoid and the humerus). Narrowing is typically seen in the setting of prior rotator cuff repair, but occasionally also results from congenital narrowing or trauma.
The structures affected are:
subscapularis tendon
long head of the biceps tendon
middle glenohumeral ligament.
Clinically, patients present with pain in the anterior aspect of the shoulder when the arm is held at the side (adducted, internally rotated and in forward flexion). The pain is characterized as deep inside and medial to the coracoacromial ligament.
This is usually resistant to conservative care and surgical treatment is usually warranted.
Surgical treatment involves a coracoplasty (removing a portion of the coracoid process) with debridement or repair of the subscapularis tear.
3. Rotator Cuff Tears
The rotator cuff is a group of tendons that connects the four muscles of the upper shoulder to the bones. The strength of the cuff allows the muscles to lift and rotate the humerus (the bone of the upper arm). The tendons run under the acromion (part of the shoulder blade) where they are very vulnerable to being damaged. This can lead to a tear resulting in a painful, weak shoulder. A tear may result suddenly from a single traumatic event or develop gradually. When the tendons or muscles of the rotator cuff tear, the patient is no longer able to lift or rotate his or her arm with the same range of motion as before the injury and/or has significant pain associated with shoulder motion. The pain is also very common at night, often radiating down the arm.
As people age, it is normal for the rotator cuff tendon to wear and degrade. The rotator cuff becomes weak and prone to rupture or tear. A fall or wrenching injury can then result in complete rupture of the tendons. This leads to pain and weakness of the shoulder.
Thus, atraumatic degenerate tears on scanning are not uncommon. These generally do not require surgical repair. However, an injury to an intact cuff can lead to a traumatic tear – and these tears do require surgical repair. The sooner a repair is performed after injury, the better the outcomes for the patient. Therefore, early identification is important.

Identifying a cuff tear that requires referral for repair:
1. Over 40yrs of age sustaining a fall or wrenching injury
2. Pain and weakness not settling in 3 weeks
3. Confirmed tear on ultrasound or MRI scan.
Causes:
1. Injury, especially while trying to lift or catch a heavy object
2. Overuse, especially after a period of inactivity
3. Poor blood supply to an area of the cuff (which occurs with increasing age)
4. A fall on an outstretched arm
5. A gradual weakening of the tendons of the shoulder, often associated with impingement
Diagnosis:
A rotator cuff tear is best diagnosed with a scan. The type of scan depends on the local resources and skills.
Ultrasound Scan – in some cases this can be done immediately in the clinic and is accurate, dynamic and cost effective.
MRI Scan – This is more costly and less accessible, but can provide information on the quality of the muscles and other underlying structures of the shoulder.
Prevention:
o Avoid excessive overhead activities.
o Strengthen your shoulders and do not try to play or work through the pain.
Treatment:
1. Painkillers and anti-inflammatory medications
2. Physiotherapy – keeps your shoulder strong and flexible and reduce the pain and weakness
3. Cortisone steroid injections – reduces inflammation and control the pain. It is advisable to avoid repeated steroid injections in the presence of a tendon tear, as this may weaken the tendon further.
4. Surgery is required –
a. If the tear follows an injury
b. When pain and weakness is not improved with injections and physiotherapy
– The goal of any surgery is to relieve the pain and improve the shoulder strength. This requires a long period of physiotherapy in addition to the surgery.
– Surgery may be done Arthroscopically (keyhole) or Open, or a combination of the two, know as a Mini-repair.
– Some tears are too large to repair and are known as ‘Massive Cuff Tears’
Rotator Cuff Repair
A complete rotator cuff tear will not heal. Complete ruptures usually require surgery if your goal is to return your shoulder to optimal function.
A rotator cuff repair involves stitching the torn tendon back onto its attachment to the arm bone (Humerus)

This may be performed either through keyhole surgery ( Arthroscopy ) or open surgery, using sutures and bone anchors .
4. Calcific tendonitis
Calcific tendonitis refers to a build-up of calcium in the rotator cuff (calcific deposit). When calcium builds up in the tendon, it can cause a build up of pressure in the tendon, as well causing a chemical irritation. This leads to pain. The pain can be extremely intense. It is one of the worst pains in the shoulder (the other being Frozen Shoulder ).

In addition to the chemical irritation and presssure, the calcific (calcium) deposit reduces the space between the rotator cuff and the acromion, as well as affecting the normal function of the rotator cuff. This can lead to subacromial impingement between the acromion and the calcium deposit in the rotator cuff when lifting the arm overhead.
The cause of the calcium build-up in the rotator cuff is not known. It tends to be more common in people between the ages of 30-60 years of age. It does eventually disappear spontaneously, but this can take between 5 to 10 years to resolve.
Diagnosis
The calcific deposit can be seen on plain x-rays, however ultrasound scan is better to find small calcific deposits which can be missed on x-rays. Ultrasound also makes it possible to assess the size of the deposit in all directions. The clinician can also see the blood vessels around the calcific deposit.
Treatment
Treatment of calcific tendinitis involves:
1. Painkillers and anti-inflammatory medications
2. Physiotherapy – keeps your shoulder strong and flexible and reduce the irritation
3. Cortisone steroid injections – reduces inflammation and control the pain
4. The calcific deposit is injected with a salt water solution or local anesthetic and the calcium is also sucked out into a syringe
5. Surgical excision
Surgery for Calcific Tendonitis:
Surgery is required if the pain is not controlled with the methods above and/or the pain is extremely severe, with night pain.
The goal of any surgery to reduce the effects of impingement, by increasing the amount of space between the acromion and the rotator cuff tendons, which will then allow for easier movement and less pain and inflammation. The calcium deposit is also debrided and released at the same time. The operation performed is Arthroscopic Subacromial Decompression & Excision of the Calcific Deposit .
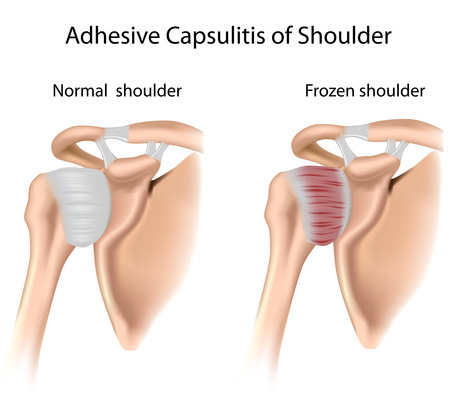
5. Frozen Shoulder
Frozen Shoulder is an extremely painful condition in which the shoulder is completely or partially unmovable (stiff). It is one of the most painful conditions of the shoulder (the others being Calcific Tendonitis or referred Nerve pain from the neck).
Frozen shoulder often starts out of the blue, but may be triggered by a mild injury to the shoulder. The condition usually goes through three phases, starting with pain, then stiffness and finally a stage of resolution as the pain eases and most of the movement returns. This process may take a long time, sometimes as long as two or more years.
Frozen shoulder may be associated with diabetes, high cholestrol, heart disease and is also seen in patients with scar tissue in their hands, a condition called Dupuytrens contracture. It may follow an injury to the shoulder or surgery.
The lining of the shoulder joint, known as the ‘capsule’, is normally a very flexible elastic stucture. It’s looseness and elasticity allows the huge range of motion that the shoulder has. With a frozen shoulder this capsule (and its ligaments) becomes inflamed, swollen, red and contracted. The normal elasticity is lost and pain and stiffness set in.
Typical Primary frozen shoulder develops slowly, and in three phases:
Freezing phase: Pain increases with movement and is often worse at night. There is a progressive loss of motion with increasing pain. This stage lasts approximately 2 to 9 months.
Frozen phase: Pain begins to diminish, however, the range of motion is now much more limited, as much as 50 percent less than in the other arm. This stage may last 4 to 12 months.
Thawing phase: The condition may begin to resolve. Most patients experience a gradual restoration of motion over the next 12 to 42 months
Treatment
If nothing is done most frozen shoulders improve significantly over 2-4 years after onset. However the pain and limitations of the stiff shoulder generally require treatment. The treatment required depends on the severity of the pain and stiffness. These include:
Physiotherapy – to prevent any further stiffness and regain range of motion
Painkillers and anti-inflammatories
Injections – reduce inflammation and provide pain reliefSurgery – Surgery has been shown to be of benefit in both the early and later stages of a Frozen Shoulder. This may involve an arthroscopic Capsular Release or Manipulation Under Anaesthetic (MUA). We prefer the Capsular Release procedure. It is excellent for both pain relief and restoring movement, with a success rate of 96% at 6 months. Intensive physiotherapy is essential after the surgery.
6. Biceps Problems
The biceps muscle has two tendons in the shoulder – the long head of biceps tendon (LHB) and short head tendon.

The LHB is approximately 9cm long and has to travel through a narrow groove at the front of the shoulder. It then has to bend through 90° to enter the shoulder joint and then attach to the labrum at the top of the glenoid. This has arisen through the process of evolution, as the human shoulder blade has moved in position from the side of our body to the back. This development has allowed us to throw but has had a few unforeseen consequences. One of these is the strain placed upon our LHB tendon.

This rather tortuous course places the tendon at a risk of inflammation. When the LHB becomes inflamed this can lead to pain at the front of the shoulder known as biceps tendonitis. Biceps tendonitis can occur on its own or be associated with rotator cuff problems both impingement and tears. Sometimes the LHB tendon in the shoulder may rupture and result in a bunching of the biceps in the upper arm, known as a ‘popeye biceps’ appearance.
Conditions affecting the long head of biceps are:
Tendonitis
Rupture.
Biceps instability (subluxation or dislocation)
The causes of biceps instability are due to:
A pulley rupture
Rotator cuff tear (subscapularis)
Fracture mal-union on non-union
Bicep tendonitis and tendinopathy sufferers will commonly report:
Pain in the region of the anterior shoulder located over the bicipital groove, occasionally radiating down to the elbow.
Overhead activities usually reproduce pain, especially those positions that combine abduction and external rotation eg cocking to throw.
The pain is often aggravated by shoulder flexion, forearm supination, and/or elbow flexion.
Some patients describe muscle weakness and clicking or snapping with shoulder movements.
A LHB rupture is denoted by a typical ‘popeye sign’ with a dropped biceps muscle. The retracted muscle may be fixed or mobile. In my experience patients with a mobile (unfixed) ruptured biceps tend to suffer with discomfort, cramping and aching from the biceps muscle with activities.
Bicipital tendinopathy diagnosis is suspected based on your symptoms, history and a clinical examination. Ultrasonography and MRI are the best investigations to confirm the diagnosis.
Treatment:
1. Physiotherapy:
Functional biceps tendonitis can occur with glenohumeral instability, as well as scapula disorders. Instability and protraction of the shoulders leads to tension on the long head of biceps tendon. This can be addressed by postural correction and a scapula setting and stabilising regime.
2. Injections (steroids, Hyaluronan, PRP):
Injections into the biceps tendon sheath are beneficial to reduce inflammation and swelling of the biceps sheath.
3. Surgery:
Arthroscopic biceps tenotomy is a good treatment for biceps tendonitis but should be reserved to elderly and low demand patients.
Biceps tenodesis is indicated for more active and higher demand patients. This can be performed as an arthroscopically assisted procedure with good strong fixation and early return to manual activities and sports.
7. Acromioclavicular Joint
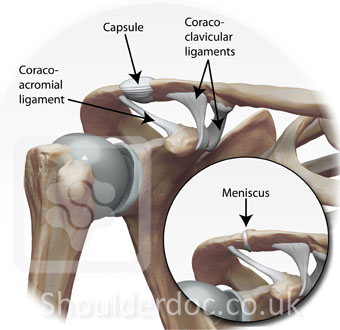
The AC joint is located at the tip of the shoulder where the acromion portion of the shoulder blade (scapula) and collarbone (clavicle) join together. The AC joint is not as mobile as the large main shoulder joint and only moves when the shoulder is overhead or across the chest (adducted). The joint is partly filled with a thick pad of cartilage, known as the meniscus, wich allows the joint to move. The AC joint is stabilised by its capsule and additional ligaments (coraco-clavicular ligaments).
Acromioclavicular Joint Arthritis
Arthritis is a degenerative disease of a joint. Thus, arthritis of the AC joint is a degenerative disease of the acromioclavicular joint or AC joint.

As a person becomes older and uses the shoulder, normal wear and tear, or degeneration, of the cartilage takes place in the joint. There is a loss of cartilage and, over time, the joint can wear out, become larger, and develop spurs (spiny projections from the bone) around the joint. This degeneration results in a condition known as osteoarthritis. Similar to arthritis in other joints of the body, there is pain and swelling in the joint as it is used. AC joint arthritis—osteoarthritis of the acromioclavicular joint—is common in middle age.
The principal cause of AC joint arthritis is use. As a person uses his/her arm and shoulder, stress is placed on the joint. This stress produces wear and tear on the cartilage, the cartilage becomes worn over time, and eventually arthritis of the joint may occur. Another cause is an old injury to the AC joint, such as ACJ Dislocation. Any activity that can put pressure on the joint, either normal or excessive, may eventually cause the arthritis condition.
Persons who must use their arms for extended periods of time are susceptible to AC joint arthritis. Constant overhead lifting, such as is engaged in by weightlifters or construction workers who work overhead, can increase the incidence of the disease. Other susceptible individuals are athletes participating in contact sports or engaging in any activity which may result in a fall on the end of the shoulder. Any blunt force to the shoulder in the course of work, household activities, or accident may cause, over time, an osteoarthritic condition of the AC joint.
Treatment:
1. Physiotherapy – to prevent any further stiffness and regain range of motion
2. Painkillers and anti-inflammatories
3. Injections into the painful joint – this usually provides good temporary relief.
4. Surgery – required for advanced disease, with pain not controlled with painkillers
Types of Surgery:
– ACJ Excision – removal of the AC joint. This may be done as an open procedure or arthroscopically (keyhole).
Prevention:
– Keep doing as much of your normal routine as possible.
– Maintain a healthy weight
– Remain active to keep muscle strength from diminishing. If you work up to a well-designed exercise program, you can keep or even improve joint flexibility.
– Keep repetitive overhead activity to a minimum
Rest only when joints are very painful.
Acromioclavicular Joint Dislocation
This injury is more common in young males. Often the result of a direct contusion to the apex of the shoulder after a fall or a forceful collision with a hard surface. It is common among football, rugby and ice hockey players as well as bicycle or motorcycle accidents. AC joint injury by indirect trauma either a fall on the elbow or a fall onto the outstretched hand may also occur. Typically in an acromioclavicular joint injury, the force initially sprains the acromioclavicular ligaments (mild sprain); then stresses the coracoclavicular ligaments (moderate sprain) and finally, if the downwards force continues, the injury progresses to tear the coracohumeral ligaments and then the deltoid trapezial fascia as well. At this point the upper extremity has lost its suspensory support and drops downwards.
Injuries to the acromioclavicular joint (ACJ) are classified on the basis of the findings from the physical examination and anteroposterior and axillary radiographs. The degree of damage to the acromioclavicular and the coracoclavicular ligaments as well as the deltoid and trapezius attachments are also considered.
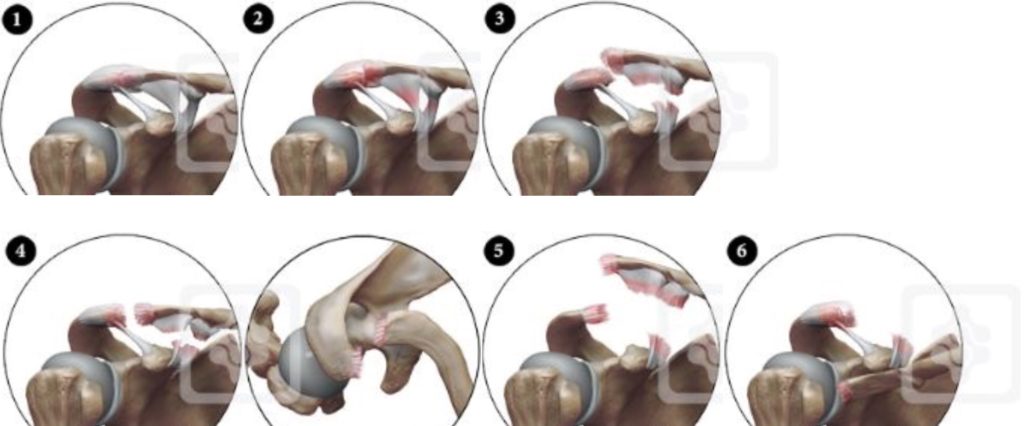
Types:
I – Sprain of acromioclavicular ligament only
II- Acromioclavicular ligaments and joint capsule.
Disrupted Coracoclavicular ligaments intact. 50% vertical subluxation of clavicle.
III- Acromioclavicular ligaments and capsule disrupted.
Coracoclavicular ligaments disrupted. Acromioclavicular joint dislocation with clavicle displaced superiorly and complete loss of contact between clavicle and acromion.
IV- Acromioclavicular ligaments and capsule disrupted. Coracoclavicular ligaments disrupted. Acromioclavicular joint dislocation and clavicle displaced posteriorly into or through trapezius muscle (posterior displacement confirmed on axillary radiograph)
V- Acromioclavicular ligaments and capsule disrupted. Coracoclavicular ligaments disrupted. Acromioclavicular joint dislocation with extreme superior elevation of clavicle (100 to 300% normal). Complete detachment of deltoid and trapezius from distal clavicle.
VI- Acromioclavicular ligaments and capsule disrupted. Coracoclavicular ligaments disrupted. Acromioclavicular joint dislocation with clavicle displaced inferior to acromion and coracoid process.
Whiplash injury to the shoulder
Whiplash injury to the shoulder is a newly recognized problem in patients who developed shoulder symptoms as a consequence of indirect trauma sustained in a car accident (Wallace et al., 1998; Levy et al., 2002). These patients usually have an established episode of trauma usually involving the shoulder wearing the seatbelt at the time of the accident. The injury originates from the whiplash movement of the shoulder where the clavicle and the body are retrained by the seatbelt. Most of these patients will have some form of soft tissue injury to the neck as well. The injuries to the shoulder may involve acromioclavicular joint subluxations and dislocations (mainly type 1 and 2).
Type I & II
Although the majority of patients with Type I and II injuries will recover and most of the acute symptoms will subside with 7-10 days of injury, these injuries are not as benign as thought. Literature review revealed a surprisingly high rate of complications (need for further surgery, pain, radiographic changes) after grade I and II AC joint sprain treated conservatively. This is in contradiction with the common perception, which suggests that grade I and II AC sprains have a good prognosis and are not associated with joint instability. Grade I and II injuries may cause persistent pain and late radiographic changes. Major symptoms, such as severe pain and instability forcing the individual to give up sports and diminish performance, was up to 9% for grade I injury and up to 42% for grade II injury. Radiographic changes were noted in 70% of patients with grade I AC joint sprains and in 75% of patients with grade II sprains. An incidence of distal clavicular Osteolysis of 6% after an AC joint separation (grade I-III) has been reported. Residual laxity was found in 33%. Some patients may also have significant weakness in horizontal abduction. A sprain may cause tears of the capsule ligaments and lesions of the meniscus and the articular cartilage. Therefore, degenerative changes due to repetitive trauma may occur.
After AC joint sprain, the torn capsular ligament can be trapped within the joint and loose pieces of articular cartilage can be released. Incongruity in the AC joint after grade II injuries may cause late symptoms. The painful symptoms may be related to instability of the AC joint, which may lead to articular degeneration after repetitive use.
The severity of grade I & II AC joint injuries is underestimated and may lead to more chronic disability than previously recognised, especially in athletes and heavy labourers who stress their shoulder daily. Some late surgery as AC joint resection arthroplasty may be needed. However, more than 50% of the patients having a good or excellent shoulder 6 years after injury.
Type III-VI
The same complications may apply to the more severe AC joint injuries. Furthermore, AC joint instability symptoms may persist, with impingement symptoms secondary to the drop down of the shoulder and the abnormal biomechanics. Patient may complain of severe deformity in the AC joint and traction symptoms with neck pain and neural brachial plexus symptoms. There is significant decrease (24%) in horizontal abduction strength at fast speeds. However, overall 87% with type III dislocation showed satisfactory outcome with conservative treatment.
Treatment:
A complete AC joint dislocation that is still painful after about 3-6 months is usually an indication for stabilisation of the joint. However, some acute dislocations that are very displaced are stabilised soon after the injury.
Acromioclavicular Joint Stabilisation – LARS Ligament for ACJ
Ligaments used to repair the ACJ need to have capacity to bear the heavy load of the upper limb, thus it is important that they have adequate structure and biomechanical integrity to act as a scaffold while the tissue regenerates. Due to complications and poor outcomes with past techniques, most surgeons are now advocating to anatomically reconstruct the coracoclavicular ligaments. Studies have shown that anatomical reconstructions better match the stiffness of the native coracoclavicular ligament and gives better results than with past non-anatomic methods.
The LARS ligament reproduces the anatomy and mechanics of the torn coracoclavicular ligaments and acts as a reinforcement to allow the coracoclavicular ligament to heal and grow into the synthetic fibres. They allow immediate mobilisation with no material through the joint. The fixation is via two bony tunnels and not an “over-the-top” approach, thus reducing clavicular erosions. The use of loop techniques offers the possibility of an earlier return to work especially in younger, active patients or ones with a high-grade dislocation.
8. SLAP Lesions
The shoulder is a ball-and-socket type of joint and is anatomically referred to as the gleno-humeral joint, describing the two bony structures involved. The socket is the glenoid cavity, a cup-shaped piece of bone that juts out from a corner of the shoulder blade (scapula). The rim of the glenoid is formed by cartilage called the labrum. The ball that fits into the socket is the head (upper part) of the humerus (arm bone).
The upper (superior) part of the labrum anchors one of the two tendons of the biceps muscle . The feature that makes SLAP possible is the way the upper biceps tendon hooks over the head of the humerus. If the arm is forcefully bent inward and twists at the shoulder, the humeral head acts as a lever and tears the biceps tendon and labrum cartilage from the glenoid bone in a front-to-back (anterior-posterior) direction. And that is how the name SLAP is derived – Superior Labrum Anterior-Posterior.

Causes and Risk Factors
Often an initial forceful movement of the labrum attached to the biceps tendon to be torn away from the bone (glenoid). This may be associated with a Dislocation of the joint, but commonly occurs in sportsmen with a pull on the arm, weightlifting, throwing injury or tackle. If the initial condition does not heal properly, pain will result and worsen over time.
The typical symptoms are pain at the top of the shoulder, clicking and pain with overhead activities. These may be confused with AC Joint problems , but athletes with SLAP tears have pain with eccentric biceps loading (such as going down in a bench press). AC Joint pain is usually felt when pressing out at the end of a shoulder or bench press.
Risk Factors: Overhead and contact sports pose a greater risk of labral tears (SLAP lesions).
Types of SLAP Tears – Depending on the type and severity of injury, the labrum will tear in different ways and degrees. These are classified as a guide to treatment.
Treatment
Painkillers and anti-inflammatories – help control the pain
Surgery is recommended if an athlete wants to continue their sports and training – SLAP lesions are repaired by keyhole surgery (arthroscopically) through 2 or 3 small incisions. Some SLAP lesions can be simply debrided and cleaned, whilst most need repairing depending on the severity of the lesion. The associated lesions are also treated such as labrum and ligament lesions with Instability.
Prevention
Strong shoulder muscles remain the best defence against shoulder injuries. Exercises that build up these muscles around the shoulder should be done. Adequate warm-up before activity and avoidance of high-contact sports will help prevent of an instability-causing injury.
9. Fractures
Fractures of the proximal humerus
Fractures of the proximal humerus are common, accounting for 5% of all fractures. These fractures tend to occur in older patients who are osteoporotic.

The most common mechanism for these fractures is a fall on the outstretched hand from a standing height. In younger patients, high-energy trauma is the cause of injury.
The treatment objective in proximal humerus fractures is to allow bone and soft tissue healing in a normal anatomical position to maximise function of the upper extremity.
Most fractures are minimally displaced and stable, so surgical fixation is not required. A supportive sling followed by early rehabilitation and have good functional outcomes.
Displaced fractures require reconstuction, because if left untreated will have a high likelihood of producing limited function.
The most common definition of displacement is 1 cm between fragments or 45° of angulation between fracture fragments. The parts that most commonly produce these fragments are the humeral head, the greater and lesser tuberosities, and the surgical neck.
The fracture pattern can be complex and difficult to assess adequately with plain x-rays, so a CT scan may be required to better understand the severity of the fracture.
The decision for surgery and the surgical methods require a skilled and experienced surgeon and a motivated patient. The personality of the fracture (eg, bone quality, fracture orientation, concurrent soft tissue injuries), the personality of the patient (eg, compliant, realistic expectations, mental status), and the personality of the surgeon (eg, surgical experience, technical familiarity, available resources) all have a tremendous effect on specific treatment indications.

The overall prognosis from proximal humerus fractures depends on numerous factors, including the following:
Type of fracture (Neer type)
Age of the patient
Overall health status of patient
Patient’s expectations
Willingness of the patient to undergo lengthy rehabilitation
Ability to restore stability of the fracture with anatomic restoration in surgically treated fractures
Clavicle Fractures
The clavicle (collarbone) is the prominent bone on either side at the front of your shoulders and top of chest. The clavicle is the only bony link between the shoulder and the body itself, as well as providing protection to important underlying blood vessels and nerves.

Clavicle fractures make up 5% of all fractures, so are not uncommon. It is a common injury in contact sports (rugby, martial arts) and impact sports (such as horse and motor racing).
A clavicle fracture is sustained by a direct blow to the clavicle, such as in a fall or accident.
Treatment:
Most clavicle fractures are mainly treated in a sling for about 4-6 weeks. Clavicle braces may provide more comfort if applied correctly and align some fractures in a more stable position. However complete healing can be slow and may take up to 3-6 months. After 6 months about 15% of clavicle fractures still may have not healed. This is known as a “nonunion”.
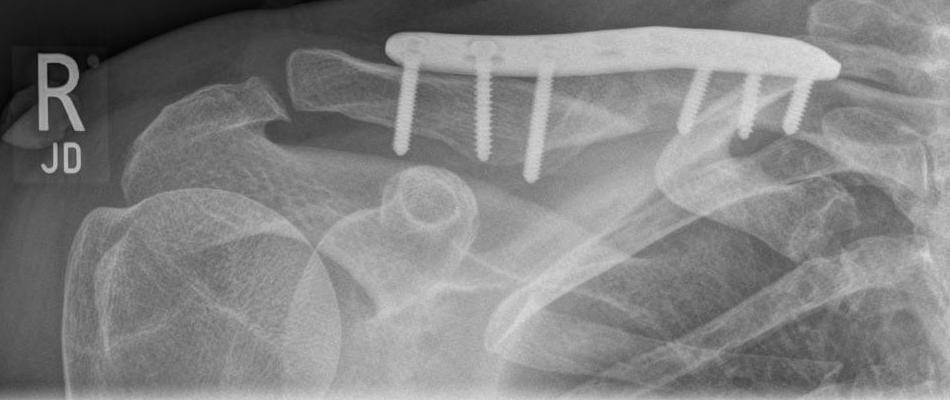
(Patient with clavicle nonunion treated with open reduction, internal fixation – plate, screws and bone graft from iliac crest)

Early fixation of clavicle fractures has some advantages, such as:
- Earlier return to work and activities
- Less pain (a the fracture is stabilised)
- Better chance of healing (as the bone ends are lined up together)
- Less chance of deformity (mal-union)
However, there are potential complications, which include:
- risk of infection
- risk of numb patch below scar
- possible scar problems (which could be cosmetically unattractive)
- failure of fixation
Therefore, the decision to perform surgery is not undertaken lightly. A surgeon may be more likely to offer early surgery in the following circumstances:
- multiple fractures
- associated scapula fracture ( floating shoulder )
- open (compound) fracture
- associated nerve or blood vessel injury
- very displaced fracture (tenting the skin)
- overlap of the fracture ends causing shortening of the clavicle
- high velocity injury with multiple bone fragments (comminuted)
- professional sports person
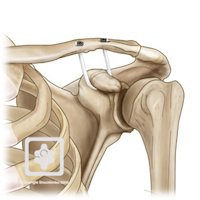
The standard method of fixation is a rigid plate and screw fixation. New plates are designed specifically for the clavicle and are low profile and very strong. This allows early mobilisation and other advantages over the older systems. Nailing of the clavicle is a technique suitable for more simple, less displaced and lower velocity clavicle fractures. It is particularly suitable for growing children and adolescents. A second operation is required to remove the nail.
Clavicle Nonunion
If the clavicle has not healed by 3 months it is called a ‘nonunion’. These are usually painful and require surgical fixation.
The surgery involves fixing the clavicle with a plate and screws, plus adding bone graft to aid the healing.
Clavicle Malunion
If the clavicle heales in a displaced position, this is called a ‘malunion’. This is accompanied by a step (deformity) in the clavicle.
This can lead to ongoing shoulder problems, especially in athletes and manual workers. Significant shortening of the clavicle can alter the normal alignment of the shoulder girdle leading to dysfunction with high demand activities.
10. Arthritis of the Shoulder
10. Arthritis of the Shoulder
Osteoarthritis is a progressive degeneration of the joints. It results when the protective surface (cartilage) that allows the joint to move smoothly is damaged. Over time this cartilage is worn away and adjacent bones are remodeled as the joint becomes increasingly abnormal and ‘rusty’, resulting in pain and stiffness.

Osteoarthritis of the shoulder is less common in comparison to many other joints, principally the hips, knees, and hands. It is nonetheless a debilitating problem and can have a significant impact on the patient’s life.
Possible causes
Traditionally thought of as a ‘wear and tear’ phenomenon the cause of osteoarthritis is generally unknown however several contributing factors have been identified these include; prior shoulder surgery, history of trauma, inflammatory conditions (mainly Rheumatoid arthritis), and shoulder overuse. Individuals particularly at risk are those who engage in high intensity overhead activities such as weightlifters and racquet sport players.
Rheumatoid arthritis is a widespread disease found throughout the body in which the patients own immune system mistakenly attacks the joints causing widespread inflammation and damage.
Symptoms
Patients with arthritis of the shoulder will classically complain of a stiff and painful shoulder, with a limited range of movement. Description of pain and stiffness that intensifies with use is common as is painful interruption of sleep. “Catching” and “noise” heard during movement is another routine finding.
Diagnosis
Osteoarthritis is usually diagnosed by a combination of clinical examination and history of the presenting complaint. Prior to proceeding with treatment, X-rays may be taken to evaluate the extent of any damage which may be helpful in deciding upon the most suitable treatment. Similarly a CT scan of the shoulder may also be requested if it is decided that surgical management would be the most appropriate option.
Treatment:
Non-operative Management
Non-operative treatment should always be exhausted prior to proceeding with any form of surgery. Possible non-operative options available include:
Physiotherapy – to prevent any further stiffness and regain range of motion
Painkillers and anti-inflammatories – mild/ moderate pain killers and anti-inflammatory medications may be taken to provide symptomatic relief. However these drugs are in no way curative and will not alter the course of the disease.
Injections – mainly short-term benefit only
Steroid injections – are often given to provide short-term relief to the patient, though this period is unpredictable due to the wide variability of the disease. Repeated injections should not be given as a long term cure as they can cause further damage to the joint.
Hyaluronan injections have been shown to be beneficial for early arthritis and where surgery is contraindicated. They seem to provide longer benefit than steroid injections with less side-effects.
PRP injections
Surgical Management
The form of surgery chosen should be the least invasive approach required to provide long term pain relief and restore function.
Arthroscopic Treatment
Arthroscopic treatment of the shoulder for osteoarthritis is primarily a temporary therapy in which the joint is “tidied up.” The surgeon removes unwanted material and smoothes off the joint, hopefully providing relief of symptoms. As mentioned previously this procedure typically provides relief for a limited time only after which more definitive measures i.e. arthroplasty are required, it’s role is therefore limited (mainly to the young).
Shoulder Replacement
Ultimately in cases of severe non-resolvable pain or previous failed treatment options, shoulder replacement (arthroplasty) is indicated. There are a number of variations of shoulder replacements available, some more invasive than others. The choice of replacement depends on a number of criteria these include: your surgeon’s preference, age, activity level, form of arthritis, and the amount of bone affected.
Traditionally the two forms of replacement that have been used are; hemiarthroplasty and total shoulder arthroplasty.
Hemiarthroplasty involves a prosthetic metal implant being placed into the upper bone in the arm (humerus) which forms half of the shoulder joint.

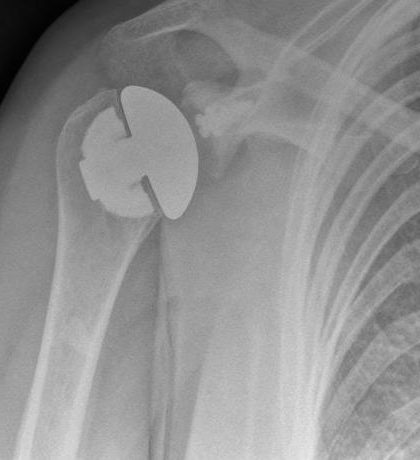
Whilst in total shoulder arthroplasty both sides of the joint are replaced. There are 2 types of total shoulder replacement, anatomic and reverse.
- Anatomic Total Shoulder Replacement
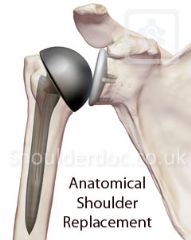
(New generation Stemless Anatomic Total Shoulder Replacement)

- Reverse Shoulder Replacement

(Rotator cuff deficiency treated with Reverse Shoulder Replacement)


(Avascular necrosis of humeral head (old fracture) treated with Reverse Shoulder Replacement)


An alternative joint reconstruction is humeral head resurfacing. In this procedure a small amount of the affected bone is removed from the humeral articulating surface (head) and replaced by a smooth metal cap. This is a particularly good treatment for active young patients as it typically provides good relief and is easy to revise if the condition deteriorates in the future.
- Humeral Head Resurfacing Arthroplasty – Copeland

(45 year old patient with shoulder osteoarthritis, unaffected glenoid, treated with Resurfacing Arthroplasty – Copeland)


Prevention:
– Keep doing as much of your normal routine as possible.
– Maintain a healthy weight
– Remain active to keep muscle strength from diminishing. If you work up to a well-designed exercise program, you can keep or even improve joint flexibility.
– Keep repetitive overhead activity to a minimum
– Rest only when joints are very painful.